View as pdf
A later version of this article appeared in Nurse Leader, Volume 21, Issue 6, December 2023.
Nursing shared governance (SG) provides an opportunity for alignment between frontline team members and nursing leadership. A Department of Nursing had a mature SG program with many thriving departmental-based SG groups. However, structural processes and guidance for unit-based SG groups were lacking and demonstrated a need for improvement. The General Theory of Effective Multi-Level Shared Governance (GEMS) framework provided an opportunity to refocus and improve Unit Practice Councils (UPC). Results demonstrated that UPC leadership competencies can be improved through focused 1:1 leadership coaching by identifying a UPC’s area of opportunity and utilizing evidence-based tools and resources.
Organizations have adopted shared governance structures over the past 40 years to drive empowerment at the frontlines of nursing care.1 SG creates a structure that allows for professional autonomy, control of nursing practice, and ultimately communication.2 Studies have demonstrated improvement in patient outcomes such as falls with injury and a reduction in hospital-acquired infections in areas that have SG in place.1 In addition, staff engagement and satisfaction have shown improvement amongst nurses who participate in SG. Improving staff morale and enhancing the way they provide care to improve patient outcomes can give a sense of belonging, which can enhance engagement across diverse areas such as inpatient, ambulatory, and perioperative settings.1 Nursing SG results in shared decision-making between nurses at all levels of an organization, a shift from the historical top-down management approach to one that is more collaborative and inclusive, allowing for open communication, discussion, and action around change. Creating and implementing these processes and structures can be challenging, and if not executed with clear expectations and guidance, can create future concerns such as ineffective and inefficient use of time, poor staff engagement, and practice variations.3
General Theory of Effective Multilevel Shared Governance (GEMS)
The GEMS framework (Figure 1) is used to accelerate shared governance. GEMS help teams identify where they are, organize themselves, and then work to make meaningful changes to evolve into a more productive and effective state.4 GEMS includes nine individual competencies: skillfulness, usefulness, effectiveness, supported by management, empowers nursing and nurses, improves patient safety, improves patient care, provides leadership, and enhances professional nursing practice. These competencies are staged amongst three phases of development: foundational inputs, empowering practices, and aligning goals.4
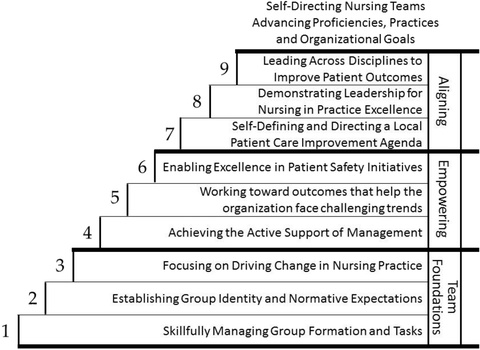
Figure 1. General Theory of Effective Multilevel Shared Governance Framework
(Reprinted with permission from Joseph ML, Bogue RJ. A theory-based approach to nursing shared governance. Nurs Outlook. 2016;64(4):339–351. https://doi.org/10.1016/j.outlook.2016.01.004)
GEMS competencies may be used to identify the focal areas of 1:1 coaching. SG paired with leadership development can promote empowering behaviors as well as enhance the overall effectiveness of the team. Providing leadership coaching creates alignment between leaders and frontline team members. Leadership must provide SG groups with time, encouragement, communication, resources, and information.5 Together leadership, coaching, and shared governance align cohesively and allow for professional development of individuals and teams.
Leadership Coaching
For SG to be successful, nurse leaders must possess effective skillsets that promote participation to improve the work environment. Organizational leaders must promote leadership development for team members of all levels, including frontline leaders.5 These structures must be in place to drive the intended behaviors and subsequent outcomes.6 As healthcare systems become more complex, nursing leaders must integrate team principles to enhance SG and foster shared decision-making.7 Leaders should ensure structures are in place to drive nurse empowerment and develop a practice environment that engages individuals to take ownership of their professional practice. To create an environment that cultivates decision-making, builds relationships, and develops accountability, there must be strong alignment from the organization.6 Leadership coaching creates a supportive environment and mentoring in this way supports leadership development.
Evidence-Based Project for UPCs
Design
The purpose of this evidence-based project was to evaluate and improve the overall effectiveness of six nursing UPCs by providing 1:1 leadership coaching to the unit leadership team. The leadership team or leaders used here references the nurse manager, assistant nurse managers, and the unit council staff nurse leaders. The project aims were to (a) improve leadership competencies, (b) improve UPC effectiveness, and (c) improve unit-based staff engagement. Six nursing units each from different divisions participated (ambulatory, behavioral health, children’s, intensive & specialty, medical-surgical, and perioperative). These units were selected because they had some type of an existing SG structure in place, but from the perspective of the division director, had opportunities for improvement. Having already established SG groups in place allowed for more time spent on development and growth instead of spending time in SG group creation.
Tools
Pre- and post-pilot data was collected utilizing two different measures: (1) staff engagement surveys and (2) Nursing Practice Council effectiveness scale (NPCes) Survey.
Staff Engagement Survey
Baseline nursing unit engagement data was collected from the 2021 annual organizational staff engagement survey. Post-pilot nursing unit engagement data was obtained from the 2022 survey. Individual item and total engagement scores were calculated by a vendor for the organization using a validated tool.
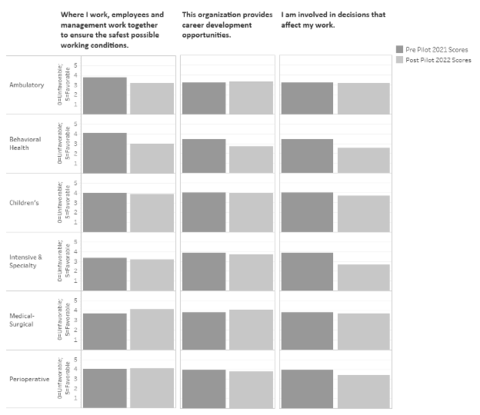
Responses for specific questions that align with the project purpose and outcomes, answered by unit nurses, were evaluated (1) I am involved in decisions that affect my work, (2) This organization provides career development opportunities, and (3) Where I work, employees and management work together to ensure the safest possible working conditions.
Nursing Practice Council Effectiveness Scale (NPCes) Survey
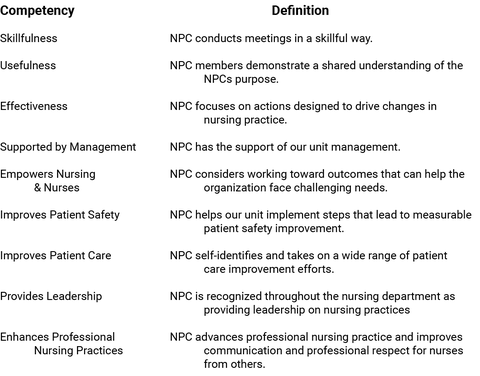
The NPCes survey tool was sent to all members of the UPC pre- and post-pilot. Some of the participating units structure their UPCs to only include nurses. Others were structured in an interprofessional approach. Regardless of the participants, the survey was sent to all members identifying as active participants of the SG group. The 21-item survey measures perceived effectiveness of the council (9 items), management (4 items), nursing leadership (4 items), and executive leadership (4 items). NPCes survey questions are answered on a 0-9 Likert scale. 0=Don’t know, 1=Not at all, 5=Quite a lot, 9=Always.8
Intervention
Pre-pilot engagement and NPCes results were collected and shared with the UPC leadership teams. The NPCes results illustrated each unit’s performance around all nine GEMS competencies (Table 1). Each competency was discussed. The unit leaders were challenged to evaluate the lowest scoring competencies and determine if they felt those were the best competencies to focus on in the coming months.
Procedure
Each leadership team identified three lower scoring competencies as areas of focus for coming six months of 1:1 coaching. Individualized, monthly 1:1 leadership coaching sessions took place for all six leadership teams, focusing on the three lower scoring competencies. Each session was approximately 60 minutes long. Evidence-based tools and strategies were identified based on the focus areas. For example, if skillfulness was a competency that was an area of focus, time was spent discussing evidence-based strategies such as creating agendas, minute taking, utilizing structured tools for record keeping, how to structure a meeting, and how to follow-up on items and share information after the meeting. If usefulness was a competency that was an area of focus, time was spent evaluating what the UPC’s expectations, norms, and purpose might be. How to define the scope of responsibility of the UPC and review of goal attainment was discussed. Key interventions such as how to set SMART goals (Specific, Measurable, Attainable, Relevant, Time-Bound) were shared. Unit leadership teams then applied the learned concepts and collaboratively implemented the evidence-based tools at the local UPC level. At subsequent 1:1 sessions, the team would discuss how the previous UPC meetings went, how strategies were applied, and identified additional opportunities for improvement going forward. After six months of focused 1:1 coaching, the same survey tools were utilized for post-pilot data collection.
Analysis and Results
Staff engagement score were analyzed by division. Mean scores were calculated and compared for improvement.
Staff Engagement Scores
Improvement was seen in 4 of 18 scores (Figure 2). The medical-surgical unit improved in all three staff engagement questions. The perioperative unit, children’s unit, and ambulatory unit improved in one of the three staff engagement questions. The intensive & specialty unit and behavioral health unit did not show improvement in any of the three staff engagement questions.
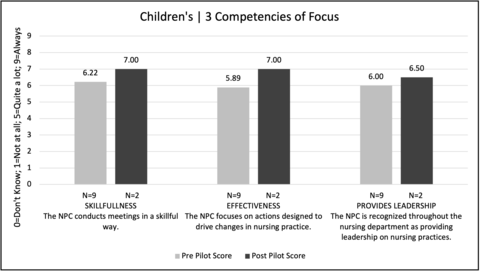
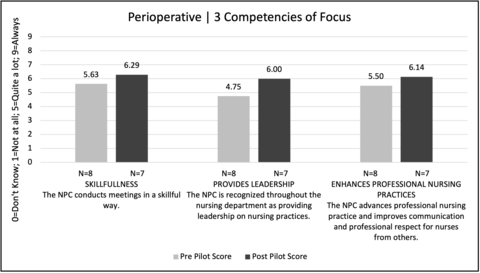
NPCes Scores
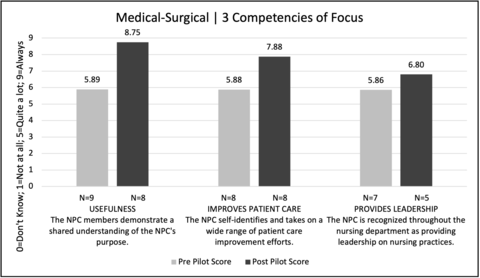
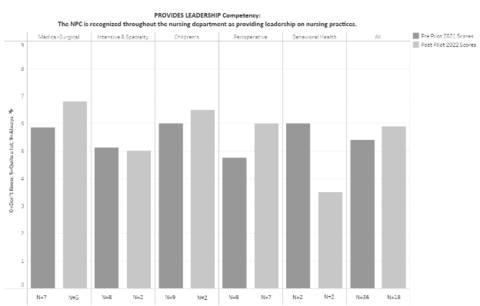
Improvement was seen in 13 of 15 scores (Figure 3-5). A subset of the NPCes participating units is being discussed, highlighting three of the five units. These three units, Medical-Surgical (Figure 3), Children’s (Figure 4), and Perioperative (Figure 5), demonstrated an improvement in each of their three focal competencies. Despite low “n” size, the medical-surgical unit demonstrated a clinically significant improvement in the usefulness and improves patient care competencies. Two units, intensive & specialty and behavioral health demonstrated an improvement in two of the three focal competencies. Interestingly, it was a project objective for all units to improve in the leadership competency as a result of focused 1:1 coaching. Four of the units (medical-surgical, children’s, perioperative, & intensive & specialty) identified the leadership competency as one of their three lower scoring competencies which was then an area of focus. Three of those four units (medical-surgical, children’s, perioperative), who focused on the leadership competency, demonstrated an improvement in the measure (Figure 6). The remaining units, who did not focus on the leadership competency during 1:1 coaching, did not show an improvement. Ambulatory unit’s post-pilot data was null and therefore not reported.
Discussion
Frontline leaders need skillsets and competencies to effectively lead frontline shared governance teams. Foundational competencies are necessary to build upon to drive empowerment and organizational alignment. Dedicating time with unit leaders to build effective UPCs is achievable utilizing the GEMS framework (Figure 1). UPC leadership competencies can be improved through focused 1:1 leadership coaching. Identifying a UPC’s area of opportunity through the NPCes tool and utilizing evidence-based tools and resources that can assist them in improving is an effective intervention. A limitation of this project was that several unit’s sample sizes were low, particularly in the post-pilot. Additional project work should be completed to continue to improve UPCs. There should be additional effort to improve survey response rates and expand the survey distribution to more individuals, perhaps to the entire unit staff. While results varied, this pilot project demonstrates improved unit council competencies in all units. In addition, certain elements of staff engagement also improved.
Implications for Executive Nursing Leaders
Executive nursing leadership cannot lose sight of the importance of the impact SG can have on both team members and patients. Ensuring team members have dedicated time away from the bedside to participate in SG is essential. The nursing workforce landscape is shifting in front of us. We must find evidence-based interventions and innovative ways to engage team members in SG and enhance our frontline leader’s abilities in leading these groups. Executive nursing leaders should recognize the value leadership coaching has on frontline leaders and be willing to invest the time and resources to develop them. In addition, as units embark on the unit-based SG journey, they should recognize the value structure and processes have on the overall success of the group.
Utilizing the GEMS framework can provide the foundational attributes needed for future success. Nurse Executives should recognize the power shared governance can have on alignment between themselves and the front-line team members, building that bridge between the two. Improving the alignment between these two can help organizations achieve goals and push the profession of nursing forward.9 Most nursing leaders today are focused on improving the patient experience, patient outcomes and staff engagement. Investing and prioritizing effective UPCs, with a focus on structural empowerment, may serve as the conduit to impact many organizational outcomes.10
References
- Kutney-Lee A, Germack H, Hatfield L, et al. Nurse engagement in shared governance and patient and nurse outcomes. J Nurs Adm. 2016;46(11):605-612.
- Kyytsönen M, Tomietto M, Moona H, Kanste O. Research on hospital-based shared governance: A scoping review. International Journal of Health Governance. 2020;25(4):371-386.
- McKnight H, Moore SM. Nursing shared governance. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022, September 19.
- Joseph ML, Bogue RJ. A theory-based approach to nursing shared governance. Nurs Outlook. 2016;64(4):339-351.
- dos Santos JL, Erdmann AL, de Andrade SR, de Mello AL, de Lima SB, Pestana AL. Governança em enfermagem: revisão integrativa da literatura [Nursing governance: An integrative review of the literature]. Rev Esc Enferm USP. 2013;47(6):1417-1425.
- Porter-O’Grady T, Clavelle JT. The structural framework for nursing professional governance: Foundation for empowerment. Nurse Leader. 2020;18(2):181-189.
- Kennerly S. Perceived worker autonomy: The foundation for shared governance. J Nurs Adm. 2000;30(12):611-617.
- Bogue RJ, Joseph ML, Sieloff CL. Shared governance as vertical alignment of nursing group power and nurse practice council effectiveness. J Nurs Manag. 2009;17(1):4-14.
- Joseph ML, Bogue RJ. C-suite roles and competencies to support a culture of shared governance and empowerment. J Nurs Adm. 2018;48(7-8):395-399.
- Speroni KG, Wisner K, Ober M, Haines F, Walters C, Budhathoki C. Effect of shared governance on nurse-sensitive indicator and satisfaction outcomes by Magnet® recognition status. J Nurs Adm. 2021;51(7-8):379-388.